
Chondromalacia Patella - Where Pain Referral Meets Function
Chondromalacia patella is a condition involving inflammation and possibly damage to the surface of the cartilage beneath the kneecap. In the early stages, there may be softening of the cartilage and a regional inflammatory response without serious damage. Left unchecked, the articular track and/or the patella itself may become fissured, pitted, and worn away.
Even in the early stages, there is likely to be fluid effusion around the knee as the body mobilizes the immune system in an attempt to repair the damaged tissues. Once fluid develops, there will be a loss of pain-free range in the knee joint, and the body will begin to stabilize the region with taut fibers and trigger points in the surrounding muscle fibers.
I encountered this issue personally a few years back, and more recently. My knee swelled up, was painful, and I found it impossible to bend my knee joint fully without experiencing intense pain. This posed a significant issue for me, particularly because my job often required me to kneel on the floor.
Initially, I was perplexed by the severe inflammation in my knee since I was very active, practiced yoga, and had never previously faced any knee problems. Normally, I could kneel and flex my knee fully for long periods without discomfort.
At the onset, I had been spending a lot of time sitting at a computer. I compared notes with my co-instructor, Doug Ringwald, who was experiencing a milder version of the same thing, more characterized by medial knee pain and less fluid effusion. Doug was also working on the courses and sitting a lot.
Gradually, we unraveled the mystery by applying the fundamental principles of Coaching The Body®, discovering an intriguing case of how function and satellite referral intersect, causing seemingly mysterious and severe issues.
Satellite Referral
Satellite referral, first articulated by Travell & Simons in their seminal Trigger Point Manual, was a relatively new theory and initially applied to only a few muscles. Regrettably, in the more recent, condensed edition authored by others, satellite referral has been largely overlooked, not receiving the attention it deserves.
During the development of CTB, I uncovered extensive clinical evidence indicating that satellite referral impacts more muscles than Travell & Simons initially thought. We have documented satellite patterns contributing to many prevalent pain conditions over the years, and teach these patterns as part of our regional pain protocols.
Satellite referral might seem enigmatic. Even the basic mechanism of pain referral is challenging to elucidate scientifically, yet it's undeniable that it occurs throughout the body. Satellite referral exists when the pain referral pattern of one muscle overlays another muscle's fibers, instigating trigger point development and dysfunction within it.
We've discovered that satellite referral often operates undetected. Latent trigger points, although not actively causing pain, can significantly influence chains of unrelated muscles through satellite referral, with pain often only manifesting at the chain's end.
The Direct Referral Trap
This scenario often misleads trigger point therapists, focusing solely on the final stage where pain is perceived, a phenomenon I refer to as the direct referral trap.
For example, front of shoulder pain is frequently reported, and Travell and Simons identify the infraspinatus as the primary source of direct referral to this region. However, treating the infraspinatus alone seldom works due to its probable role in satellite referral and its complex functional relationships with other muscles.
For further details, my book, ENDING PAIN, delves deeper into this topic. For current purposes, our focus is on a particular satellite pattern pivotal for understanding the development of chondromalacia patella.
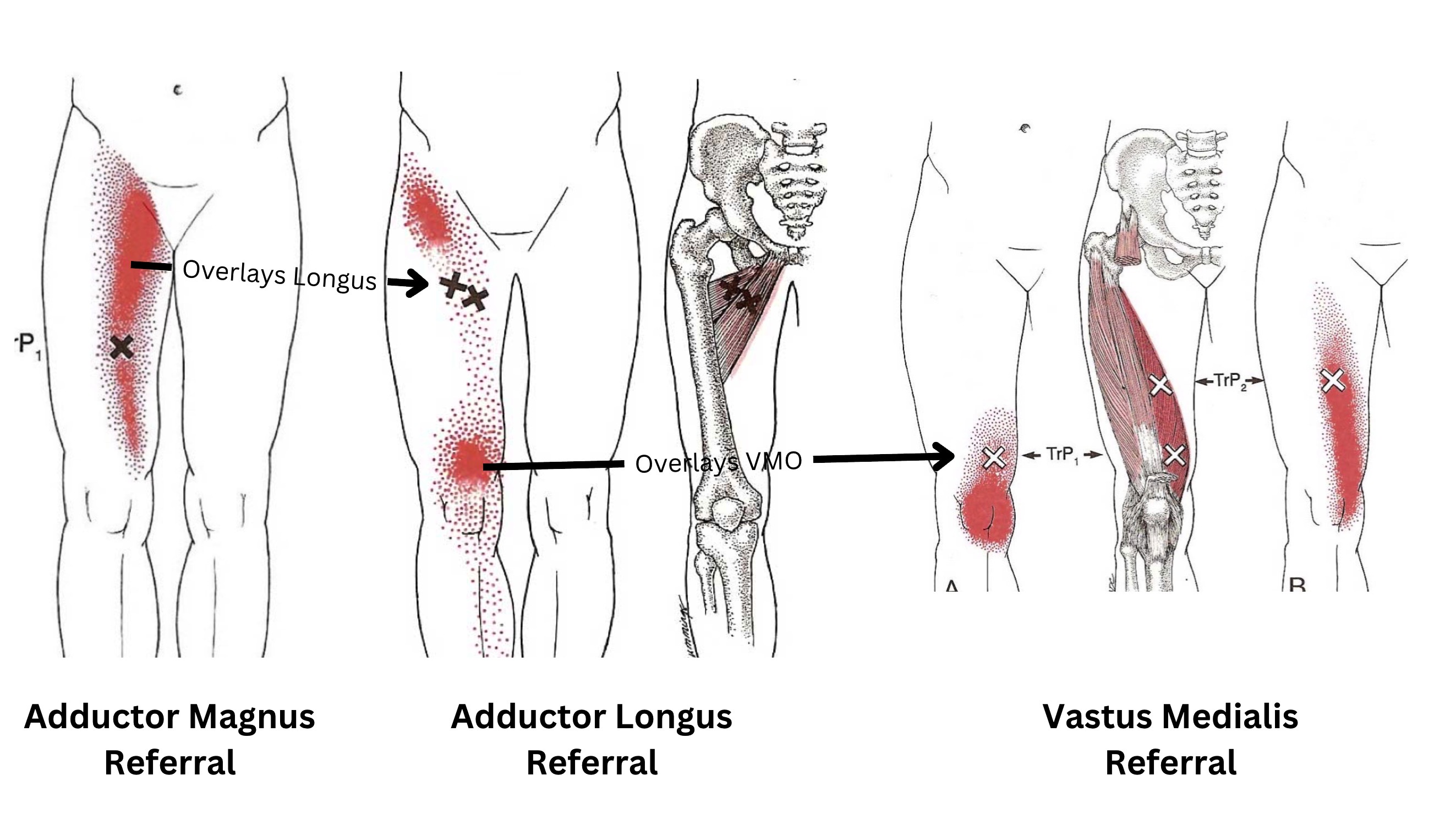
In Doug’s case, even without a lot of fluid effusion he would experience medial knee pain. This is most often caused as a direct referral of the medial quadriceps, the vastus medialis.
We found that we could trigger his medial knee pain by applying compression to an area of the adductor magnus. This is a clear case of satellite referral. The adductor magnus referral zone lies directly over adductor longus as well as portions of the vastus medialis, but does not directly refer to the knee itself.
Adductor longus also has a distal referral over the oblique belly of vastus medialis, and these fibers are well-known to induce medial knee pain.
Where Referral Meets Function
Any muscle that has developed taut fibers and trigger points is likely to exhibit issues beyond referred pain. Taut fibers, even if they harbor latent trigger points, often compromise strength as well as smooth, uninhibited contractile behavior.
Muscle inhibition, a term frequently used yet seldom actually understood, refers to a muscle's failure to activate in a timely manner or with sufficient strength, causing distorted movements or posture. Notable muscles affected by inhibition include the low trapezius and, relevant to our current discussion, the vastus medialis.
Muscles do not recruit fibers uniformly upon activation. Larger fibers typically activate after the smaller ones, which, in postural muscles, allows for chronic posture maintenance without excessive energy consumption.
The oblique section of the vastus medialis plays an essential role in keeping the kneecap aligned. It must counterbalance the vastus lateralis' pull on the quadriceps tendon, ensuring the kneecap remains centered in its track during quad engagement.
If the medialis does not activate early enough, the vastus lateralis fibers will misalign the patella toward the track's outer wall, setting the stage for chondromalacia patella.

Assessing faulty tracking is straightforward (refer to the accompanying video) by watching the patella's path as the quads start to engage with minimal effort. Early on, the smallest VMO fibers must counteract the vastus lateralis' oblique tug.
In cases of chondromalacia, the medialis fibers often remain inactive as the first vastus lateralis fibers activate, causing the patella to shift laterally before moving upwards.
I recently had a recurrence of inflammation and swelling in my right knee, and in the video I show an assessment which clearly shows faulty tracking when I slowly engage the quadriceps without any manual compression on muscles.
What is fascinating is that as soon as I provide vibration and distraction on the VMO fibers, they are able to fire and the tracking corrects in real time. Even more revelatory is that the same thing occurs with vibration on the adductor longus and then the adductor magnus.
The adductors don’t have a significant force contribution to the oblique pull of the VMO on the quadriceps tendon, so this can only be explained via a neurological disruption of satellite referral. It demonstrates clearly that satellite referral has a role in the neurological defacilitation of the muscle, and manual compression temporarily turns this off. We exploit this property extensively in the CTB manual therapy system.
Medical researchers have observed a link between 10-15 ml of fluid effusion and vastus medialis defacilitation - however, this is likely a co-occurrence rather than a causative relationship. In the absence of a working model of trigger point formation altering muscle behavior, it may just be an attempt to find a physiological reason for the vastus medialis refusing to fire.
Addressing Chondromalacia Patella
The internet is full of various techniques that are supposed to correct firing order, engage and strengthen the VMO specifically (both highly questionable physiologically) and so on, but these strategies are all flawed because they fail to recognize the role of trigger points in general, and satellite referral specifically in causing “firing order” dysfunction.
More importantly, simply treating the VMO is a case of “shooting the messenger”. It’s the end of a chain. You must discover the true origin of the issue, and the medial quad is unlikely to develop dysfunction in a vacuum, unless there is some specific lifestyle issue that is stressing the quads.
Overuse syndromes would tend to affect the quads equally, so this is a poor explanation for vastus medialis dysfunction in any case. More significantly, quads are prime satellite referral targets on both the medial and lateral sides from large hip muscles like the adductors and glutes.
During the normal activities of life, the quads are less likely to be stressed, whereas the glutes and adductor magnus are very sensitive to disturbances in gait caused by issues like hyperpronation or leg length discrepancy. This makes for a much more rational explanation than medial side knee pain appearing out of nowhere.
Too much sitting on insufficiently padded surfaces maintains static compression on the high adductor magnus and glute max fibers, which over time causes stagnation and trigger point formation.
I have achieved excellent, repeatable and quick results with this condition by analyzing and treating the true source via chains of satellite referral. None of the other theories can explain why the adductor magnus plays such a clear tole in this condition, because they don’t acknowledge the clinical importance of trigger points and hidden networks of satellite referral.

Our treatment approach for chondromalacia patella and patellofemoral pain syndrome is multi-faceted:
- The CTB Core Protocol for Lower Body Pain quickly restores function in the various muscles that contribute directly or indirectly to patellar alignment. This can be implemented via bodywork, self-care and/or corrective exercise supported by the use of therapeutic percussion. The analysis and treatment of many knee conditions is thoroughly covered in our online CTB Foundation Bundle.
- I use kinesiology tape to assist the compromised VMO fibers in keeping the patella medially displaced to minimize disturbance to the articular surface due to the asymmetric lateral pull of the VL.
- Non-ballistic exercise and movement helps to quickly restore the proper functioning of the VMO and adductors. Examples include biking, light kettlebell swings, and unloaded squats.
- Topical and systemic anti-inflammatories will help the articular surfaces and connected tissues return to normal.
- To prevent re-occurrence, you can minimize compression of the adductor magnus while sitting by providing proper cushioning in desk chairs. I have found sheepskin to be an effective natural pad that helps a great deal.
Using these strategies, I quickly reduced inflammation and regained normal knee joint function in a relatively short span during my recent symptom flare-up. Although the sudden onset of chondromalacia can be alarming, it can be just as swiftly resolved with the correct knowledge.
Get Our Free Guide For Manual Therapists

Most pain is referred by trigger points in muscles, although most medical professionals don’t understand this, and are misled by the “illusion of injury”.
The truth is, most pain can be eliminated fully and efficiently by understanding its true origins using the Coaching The Body principles and techniques.
With my foundations online courses and membership, you’ll learn how to eliminate pain and be supported in our robust CTB Mastermind community.
Subscribe to Coaching The Body® Blog and get the latest posts in your email.
All Posts





Subscribe to Youtube
